Upper Limb
This document was uploaded by user and they confirmed that they have the permission to share it. If you are author or own the copyright of this book, please report to us by using this DMCA report form. Report DMCA
Overview
Download & View Upper Limb as PDF for free.
More details
- Words: 2,461
- Pages: 12
Functional Anatomy of the Upper Limb Bill Sellers Email: [email protected] This lecture can be found at: http://mac-huwis.lut.ac.uk/~wis/lectures/
In previous lectures you have learnt about the general principles of musculoskeletal function. This lecture will cover specific details of the functional anatomy of the upper limb to illustrate the points made previously and as useful information in its own right. In the course of the lecture I will move distally down the limb from the pectoral girdle to the phalanges. This is not an exhaustive coverage but will cover the main functional anatomical features of the joints and musculature including ranges of movement and the major actions of the muscles.
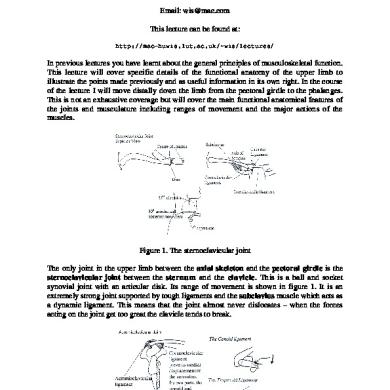
Figure 1. The sternoclavicular joint The only joint in the upper limb between the axial skeleton and the pectoral girdle is the sternoclavicular joint between the sternum and the clavicle. This is a ball and socket synovial joint with an articular disk. Its range of movement is shown in figure 1. It is an extremely strong joint supported by tough ligaments and the subclavius muscle which acts as a dynamic ligament. This means that the joint almost never dislocates – when the forces acting on the joint get too great the clavicle tends to break.
Figure 2. The acromioclavicular joint Moving distally the next joint is the acromioclavicular joint: a sliding synovial joint between the acromion process on the scapular and the clavicle. Once again there are strong ligaments binding the two bones together especially the coracoclavicular ligament whose two parts have perpendicular fibres to prevent excessive movement both medially and anteriorly.
Figure 3. Movements of the scapular Between the two of them the sternoclavicular and acromioclavicular joints allow a large range of movements of the scapular as shown in figure 3. There is no specific joint between the scapular and the thoracic cage although the movements all consist of the blade of the scapular sliding around the various curves of the thoracic cage. There is no bone to bone contact though since the deep surface of the scapular is covered by both the subscapularis and serratus anterior muscles. It is important to remember that a great deal of the overall mobility of the shoulder is actually due to the mobility of the scapular. The limb girdle for the lower limb (the pelvis) is firmly fixed to the axial skeleton and so sacrifices mobility to gain increased stability and better load bearing capacity.
Figure 4. Muscles acting on the scapular With such a complex array of possible movements it should come as no surprise that there are quite a large number of muscles that act on the scapular. The main ones are shown in figure 4. These muscles do not tend to act in isolation and because they tend to be muscular sheets rather than fusiform or strap muscles the precise action depends on which fibres within the muscle are activated (this is because the fibres in sheet muscles rarely run in parallel throughout the whole of the muscle).
Figure 5. Dorsal aspect of the arm The next joint is the glenohumeral joint between the head of the humerus and the glenoid fossa of the scapula. This is a highly mobile ball and socket joint and to cope with this mobility a large number of muscles. Figure 5 shows the main extensors of the shoulder but note that triceps is also an elbow extensor and only the long head acts as a shoulder extensor.
Figure 6. Ventral aspect of the arm The flexors of the shoulder are on the ventral aspect (figure 6). Note that the very important arm flexor, pectoralis major, has additional actions (adduction and medial rotation) so that if a pure flexion is required then other muscles need to act antagonistically for adduction (e.g. deltoid, supraspinatus) and medial rotation (e.g. teres minor, infraspinatus) to prevent the unwanted actions. Similarly latissimus dorsi is a major extensor which again produces
adduction and medial rotation and would require antagonistic action in other muscles for pure extension. Latissimus dorsi and pectoralis major often act together to produce very powerful adduction since their extension and flexion components cancel each other although this would still leave the medial rotation component.
Figure 7. Superior view of the shoulder If we look down on the shoulder from above (figure 7) we can see the medial and lateral rotators, and the abductors. Deltoid is a triangular (delta) shaped muscle which has all three actions depending on which fibres you look at. Its main action is as an abductor though. Rotation is performed by the small rotator cuff muscles and as a side effect of the big abductors.
Figure 8. Shoulder abduction Shoulder abduction (figure 8) is a more complex activity than might originally be thought. If you start from the anatomical position and begin to abduct the arm the initial 10° is performed entirely by supraspinatus because initially the fibres of deltoid are in the wrong direction to help. After that the much larger deltoid takes over the work. Abduction continues for about 110° at the glenohumeral joint but subsequent abduction takes place by upward rotation of the scapular. The full range of abduction (180°) can also only take place if the arm is medially rotated.
Figure 9. The glenohumeral joint The extreme mobility of the glenohumeral joint means that it cannot be stabilised by the normal, passive elastic mechanisms of ligaments. Instead it has active stabilisation from the short muscles that surround the joint – the so called rotator cuff muscles (figure 9). You can see from the joint shape and locations of the muscles that there is little to support the joint inferiorly and indeed dislocations of the shoulder are almost always in this direction.
Figure 10. The elbow joint The elbow joint is a complex of three joints that share the same synovial sheath (figure 10). These are the humeroradial, humeroulnar, and superior radioulnar joints. The humeroradial and humeroulnar joints allow flexion and extension at the elbow whilst the superior radioulnar, humeroradial, and the more distal inferior radioulnar joints allow the specialised actions of supination and pronation. This action is a rolling of the radius around the ulna that produces an apparent rotation of the wrist around a longitudinal axis. The elbow flexors and extensors can be seen in figures 5 and 6. Triceps is the main extensor and brachialis and biceps brachii the main flexors. Biceps brachii is also a major supinator and this action stops it being an effective flexor of the pronated forearm.
Figure 11. Pronation and supination The muscles pronator teres and pronator quadratus act to pronate the forearm (see figure 11). When they contract they role the radius anteriorly across the ulna. The converse action, supination, is mainly produced by biceps brachii with some help from supinator. Biceps brachii is a much larger muscle than the other three and this means that the action of supination tends to be much stronger than pronation. Supination of the right arm is the action used to drive screws into a substrate and produces more torque than unscrewing which uses pronantion.
Figure 12 Superficial extensors in the forearm The forearm contains a large number of muscles. Dorsally these are primarily extensors of the wrist and fingers as shown in figure 12. They do attach to the common extensor origin on the lateral epicondyle of the humerus so you might expect them to have an action at the elbow but because this attachment point is so close to the centre of rotation of the elbow their effect is minimal except for brachioradialis which is actually a strong elbow flexor. Similarly there are superficial flexors in the ventral compartment (see figure 5) which originate on the common flexor origin on the medial epicondyle of the humerus whose effect at the elbow is minimal and whose primary actions are more distally at the wrist and hand. Palmaris longus is actually missing in 13% of individuals – it is a weak wrist flexor and acts to tense the palmar aponeurosis. It is therefore a prime candidate (in those of us who have one) for surgical removal for use as a tendon repair material elsewhere in the body.
Figure 13 Middle and deep flexors in the forearm The deeper muscles in the flexor compartment are extrinsic hand muscles – they are powerful flexors of the fingers. Their force is transmitted to the hand through long tendons. Somewhat oddly the deeper flexor digitorum profundus attaches more distally on the fingers than the more superficial flexor digitorum superficialis which means that the FDS tendon has to split to let the FDP tendon pass through it.
Figure 14. Middle and deep extensors in the forearm The arrangement in the extensor compartment is somewhat similar although the extensor muscles are smaller than the flexors (figure 14). Flexors are used to produce the clenched-fist power grips whereas there is not much need for forced extension.
Figure 15. Joints of the hand Moving to the hand there are a large number of complex joints at the wrist and between the fingers. These are illustrated in figure 15. The wrist consists of 10 small carpal bones but fortunately it can be functionally divided into two components: the radiocarpal and midcarpal joints. The wrist complex is usually described as a condyloid synovial joint allowing adduction, abduction (also known as ulnar and radial deviation), flexion and extension. The exact ways that the wrist bones move to produce these composite movements is complex but flexion occurs mostly at the midcarpal joint and extension is mostly at the radiocarpal joint. The radiocarpal joint also provides most of the adduction and abduction. Other joints that you can see are the carpometacarpal joints that are numbered from 1 to 5 between the distal row of carpal bones and the five metacarpals. The first CMC joint is the best example of a sellar (saddle-shaped) joint which allows flexion, extension, adduction and abduction of the first ray. The other four are under tight ligamentous control and only allow a small amount of sliding. Distally are the five metacarpophalangeal joints. This time the first MCP joint has little mobility but the other four allow flexion, extension, adduction and abduction.
Figure 16. The bones of the hand [Netter 1997]
More distally still are the simple hinge joints of the phalanges (see figure 16): the five proximal and distal interphalageal joints and the four middle interphalangeal joints since the first ray only has two phalanges.
Figure 17. Wrist cross-section [Snell 1986] When we look at the muscles that act over the wrist joint (figure 17) we get a complex picture because as well as the specific wrist muscles (FCR, FCU, ECR, ECU and PL) all the tendons from the extrinsic hand muscles also pass this joint and so have an effect depending on the relative position of their tendon to the joint centre. The primary movers of the wrist (FCR, FCU, ECR, ECU) also act the 4 corners of the joint so all produce a dual action. Thus FCR produces wrist flexion and radial deviation, FCU flexion and ulnar deviation, ECR extension and radial deviation, and ECU extension and ulnar deviation. Thus to produce pure flexion, extension, abduction or adduction requires the activation of the correct two muscles: the two flexors produce flexion together because the adduction and abduction actions cancel out etc. If finger movements are required without corresponding wrist movements then the wrist only muscles need to act antagonistically to avoid the unwanted wrist movement. You can also see from figure 17 that the median nerve shares a rather small and inextensible space with the extrinsic finger flexors. This is the carpal tunnel where tendonitis can cause swelling which presses on the median nerve producing pain and in severe cases paralysis of some of the intrinsic hand muscles: carpal tunnel syndrome.
Figure 18. Various types of grip [Aiello & Dean 1990] The primary role of the hand itself is grasping and manipulation. Figure 18 shows the variety of grips that have been classified. A and B are simple grips, C, D and E are precision grips and F, G and H are power grips. It is suggested that the precision grips are unique to humans among the primates.
Figure 19. The superficial intrinsic hand muscles [Jacob 1996] These fine movements are controlled by the intrinsic hand muscles in conjunction with the more powerful extrinsic hand muscles of the forearm. Figure 19 shows the superficial palmar (ventral) group. These are the muscles of the thenar and hypothenar eminences which move the first and fifth digits respectively. As you might imagine movements of the fifth digit are not terribly important but the relatively large thenar eminence muscles are very important for the various movements of the thumb. The first ray is rotated 90° to the other rays so that flexion of the thumb moves it medially across the palm of the hand, abduction moves it anteriorly, perpendicular to the palm, extension moves it laterally in the plane of the palm and adduction moves it posteriorly perpendicular to the palm. The special movement, opposition, is the combined flexion and adduction that brings the palmar surface of the tip of the first digit towards the palmar surfaces of the tips of any of the other four digits.
The lumbricals are muscles that attach to the tendons of the flexor digirorum profundus muscles and the extensor digitorum comunalis tendons. They allow a controlled transfer of power from the FDP to the EDC when flexing and extending the fingers and also allow flexing of the MCP joint whilst keeping the IP joints extended.
Figure 20. Palmar and dorsal interossei [Jacobs 1996] The other intrinsic muscles are the palmar and dorsal interossei. These act to abduct (palmar) and adduct (dorsal) the MCP joints of the fingers. The first dorsal interosseous muscle is very important fin pincer or pinch grips. These are shown in figure 20.
Figure 21. The extensor mechanism of the hand [Snell 1986] The tendon arrangement around the fingers is complex as illustrated in figure 21. As previously mentioned the FDP tendon pierces the FDS tendon to attach to the base of the distal phalanx and the lumbricals attach the FDP tendon to the EDC. The EDC tendon connects to the lumbricals, the dorsal interossei and to all three phalanges and is known as the extensor expansion. This arrangement allows complex movements such as the unscrewing of a pen top whilst holding the pen in one hand, but none of the movements are entirely independent because single muscles act over several joints at once. Bibliography Jacobs S. Anatomy: a dissection manual and atlas. 1996 New York: Churchill Livingston. Netter FH. Atlas of human anatomy. 1997 East Hanover, New Jersey: Novartis.
Snell RS. Clinical anatomy for medical students. 1986 Boston: Little, Brown.
In previous lectures you have learnt about the general principles of musculoskeletal function. This lecture will cover specific details of the functional anatomy of the upper limb to illustrate the points made previously and as useful information in its own right. In the course of the lecture I will move distally down the limb from the pectoral girdle to the phalanges. This is not an exhaustive coverage but will cover the main functional anatomical features of the joints and musculature including ranges of movement and the major actions of the muscles.
Figure 1. The sternoclavicular joint The only joint in the upper limb between the axial skeleton and the pectoral girdle is the sternoclavicular joint between the sternum and the clavicle. This is a ball and socket synovial joint with an articular disk. Its range of movement is shown in figure 1. It is an extremely strong joint supported by tough ligaments and the subclavius muscle which acts as a dynamic ligament. This means that the joint almost never dislocates – when the forces acting on the joint get too great the clavicle tends to break.
Figure 2. The acromioclavicular joint Moving distally the next joint is the acromioclavicular joint: a sliding synovial joint between the acromion process on the scapular and the clavicle. Once again there are strong ligaments binding the two bones together especially the coracoclavicular ligament whose two parts have perpendicular fibres to prevent excessive movement both medially and anteriorly.
Figure 3. Movements of the scapular Between the two of them the sternoclavicular and acromioclavicular joints allow a large range of movements of the scapular as shown in figure 3. There is no specific joint between the scapular and the thoracic cage although the movements all consist of the blade of the scapular sliding around the various curves of the thoracic cage. There is no bone to bone contact though since the deep surface of the scapular is covered by both the subscapularis and serratus anterior muscles. It is important to remember that a great deal of the overall mobility of the shoulder is actually due to the mobility of the scapular. The limb girdle for the lower limb (the pelvis) is firmly fixed to the axial skeleton and so sacrifices mobility to gain increased stability and better load bearing capacity.
Figure 4. Muscles acting on the scapular With such a complex array of possible movements it should come as no surprise that there are quite a large number of muscles that act on the scapular. The main ones are shown in figure 4. These muscles do not tend to act in isolation and because they tend to be muscular sheets rather than fusiform or strap muscles the precise action depends on which fibres within the muscle are activated (this is because the fibres in sheet muscles rarely run in parallel throughout the whole of the muscle).
Figure 5. Dorsal aspect of the arm The next joint is the glenohumeral joint between the head of the humerus and the glenoid fossa of the scapula. This is a highly mobile ball and socket joint and to cope with this mobility a large number of muscles. Figure 5 shows the main extensors of the shoulder but note that triceps is also an elbow extensor and only the long head acts as a shoulder extensor.
Figure 6. Ventral aspect of the arm The flexors of the shoulder are on the ventral aspect (figure 6). Note that the very important arm flexor, pectoralis major, has additional actions (adduction and medial rotation) so that if a pure flexion is required then other muscles need to act antagonistically for adduction (e.g. deltoid, supraspinatus) and medial rotation (e.g. teres minor, infraspinatus) to prevent the unwanted actions. Similarly latissimus dorsi is a major extensor which again produces
adduction and medial rotation and would require antagonistic action in other muscles for pure extension. Latissimus dorsi and pectoralis major often act together to produce very powerful adduction since their extension and flexion components cancel each other although this would still leave the medial rotation component.
Figure 7. Superior view of the shoulder If we look down on the shoulder from above (figure 7) we can see the medial and lateral rotators, and the abductors. Deltoid is a triangular (delta) shaped muscle which has all three actions depending on which fibres you look at. Its main action is as an abductor though. Rotation is performed by the small rotator cuff muscles and as a side effect of the big abductors.
Figure 8. Shoulder abduction Shoulder abduction (figure 8) is a more complex activity than might originally be thought. If you start from the anatomical position and begin to abduct the arm the initial 10° is performed entirely by supraspinatus because initially the fibres of deltoid are in the wrong direction to help. After that the much larger deltoid takes over the work. Abduction continues for about 110° at the glenohumeral joint but subsequent abduction takes place by upward rotation of the scapular. The full range of abduction (180°) can also only take place if the arm is medially rotated.
Figure 9. The glenohumeral joint The extreme mobility of the glenohumeral joint means that it cannot be stabilised by the normal, passive elastic mechanisms of ligaments. Instead it has active stabilisation from the short muscles that surround the joint – the so called rotator cuff muscles (figure 9). You can see from the joint shape and locations of the muscles that there is little to support the joint inferiorly and indeed dislocations of the shoulder are almost always in this direction.
Figure 10. The elbow joint The elbow joint is a complex of three joints that share the same synovial sheath (figure 10). These are the humeroradial, humeroulnar, and superior radioulnar joints. The humeroradial and humeroulnar joints allow flexion and extension at the elbow whilst the superior radioulnar, humeroradial, and the more distal inferior radioulnar joints allow the specialised actions of supination and pronation. This action is a rolling of the radius around the ulna that produces an apparent rotation of the wrist around a longitudinal axis. The elbow flexors and extensors can be seen in figures 5 and 6. Triceps is the main extensor and brachialis and biceps brachii the main flexors. Biceps brachii is also a major supinator and this action stops it being an effective flexor of the pronated forearm.
Figure 11. Pronation and supination The muscles pronator teres and pronator quadratus act to pronate the forearm (see figure 11). When they contract they role the radius anteriorly across the ulna. The converse action, supination, is mainly produced by biceps brachii with some help from supinator. Biceps brachii is a much larger muscle than the other three and this means that the action of supination tends to be much stronger than pronation. Supination of the right arm is the action used to drive screws into a substrate and produces more torque than unscrewing which uses pronantion.
Figure 12 Superficial extensors in the forearm The forearm contains a large number of muscles. Dorsally these are primarily extensors of the wrist and fingers as shown in figure 12. They do attach to the common extensor origin on the lateral epicondyle of the humerus so you might expect them to have an action at the elbow but because this attachment point is so close to the centre of rotation of the elbow their effect is minimal except for brachioradialis which is actually a strong elbow flexor. Similarly there are superficial flexors in the ventral compartment (see figure 5) which originate on the common flexor origin on the medial epicondyle of the humerus whose effect at the elbow is minimal and whose primary actions are more distally at the wrist and hand. Palmaris longus is actually missing in 13% of individuals – it is a weak wrist flexor and acts to tense the palmar aponeurosis. It is therefore a prime candidate (in those of us who have one) for surgical removal for use as a tendon repair material elsewhere in the body.
Figure 13 Middle and deep flexors in the forearm The deeper muscles in the flexor compartment are extrinsic hand muscles – they are powerful flexors of the fingers. Their force is transmitted to the hand through long tendons. Somewhat oddly the deeper flexor digitorum profundus attaches more distally on the fingers than the more superficial flexor digitorum superficialis which means that the FDS tendon has to split to let the FDP tendon pass through it.
Figure 14. Middle and deep extensors in the forearm The arrangement in the extensor compartment is somewhat similar although the extensor muscles are smaller than the flexors (figure 14). Flexors are used to produce the clenched-fist power grips whereas there is not much need for forced extension.
Figure 15. Joints of the hand Moving to the hand there are a large number of complex joints at the wrist and between the fingers. These are illustrated in figure 15. The wrist consists of 10 small carpal bones but fortunately it can be functionally divided into two components: the radiocarpal and midcarpal joints. The wrist complex is usually described as a condyloid synovial joint allowing adduction, abduction (also known as ulnar and radial deviation), flexion and extension. The exact ways that the wrist bones move to produce these composite movements is complex but flexion occurs mostly at the midcarpal joint and extension is mostly at the radiocarpal joint. The radiocarpal joint also provides most of the adduction and abduction. Other joints that you can see are the carpometacarpal joints that are numbered from 1 to 5 between the distal row of carpal bones and the five metacarpals. The first CMC joint is the best example of a sellar (saddle-shaped) joint which allows flexion, extension, adduction and abduction of the first ray. The other four are under tight ligamentous control and only allow a small amount of sliding. Distally are the five metacarpophalangeal joints. This time the first MCP joint has little mobility but the other four allow flexion, extension, adduction and abduction.
Figure 16. The bones of the hand [Netter 1997]
More distally still are the simple hinge joints of the phalanges (see figure 16): the five proximal and distal interphalageal joints and the four middle interphalangeal joints since the first ray only has two phalanges.
Figure 17. Wrist cross-section [Snell 1986] When we look at the muscles that act over the wrist joint (figure 17) we get a complex picture because as well as the specific wrist muscles (FCR, FCU, ECR, ECU and PL) all the tendons from the extrinsic hand muscles also pass this joint and so have an effect depending on the relative position of their tendon to the joint centre. The primary movers of the wrist (FCR, FCU, ECR, ECU) also act the 4 corners of the joint so all produce a dual action. Thus FCR produces wrist flexion and radial deviation, FCU flexion and ulnar deviation, ECR extension and radial deviation, and ECU extension and ulnar deviation. Thus to produce pure flexion, extension, abduction or adduction requires the activation of the correct two muscles: the two flexors produce flexion together because the adduction and abduction actions cancel out etc. If finger movements are required without corresponding wrist movements then the wrist only muscles need to act antagonistically to avoid the unwanted wrist movement. You can also see from figure 17 that the median nerve shares a rather small and inextensible space with the extrinsic finger flexors. This is the carpal tunnel where tendonitis can cause swelling which presses on the median nerve producing pain and in severe cases paralysis of some of the intrinsic hand muscles: carpal tunnel syndrome.
Figure 18. Various types of grip [Aiello & Dean 1990] The primary role of the hand itself is grasping and manipulation. Figure 18 shows the variety of grips that have been classified. A and B are simple grips, C, D and E are precision grips and F, G and H are power grips. It is suggested that the precision grips are unique to humans among the primates.
Figure 19. The superficial intrinsic hand muscles [Jacob 1996] These fine movements are controlled by the intrinsic hand muscles in conjunction with the more powerful extrinsic hand muscles of the forearm. Figure 19 shows the superficial palmar (ventral) group. These are the muscles of the thenar and hypothenar eminences which move the first and fifth digits respectively. As you might imagine movements of the fifth digit are not terribly important but the relatively large thenar eminence muscles are very important for the various movements of the thumb. The first ray is rotated 90° to the other rays so that flexion of the thumb moves it medially across the palm of the hand, abduction moves it anteriorly, perpendicular to the palm, extension moves it laterally in the plane of the palm and adduction moves it posteriorly perpendicular to the palm. The special movement, opposition, is the combined flexion and adduction that brings the palmar surface of the tip of the first digit towards the palmar surfaces of the tips of any of the other four digits.
The lumbricals are muscles that attach to the tendons of the flexor digirorum profundus muscles and the extensor digitorum comunalis tendons. They allow a controlled transfer of power from the FDP to the EDC when flexing and extending the fingers and also allow flexing of the MCP joint whilst keeping the IP joints extended.
Figure 20. Palmar and dorsal interossei [Jacobs 1996] The other intrinsic muscles are the palmar and dorsal interossei. These act to abduct (palmar) and adduct (dorsal) the MCP joints of the fingers. The first dorsal interosseous muscle is very important fin pincer or pinch grips. These are shown in figure 20.
Figure 21. The extensor mechanism of the hand [Snell 1986] The tendon arrangement around the fingers is complex as illustrated in figure 21. As previously mentioned the FDP tendon pierces the FDS tendon to attach to the base of the distal phalanx and the lumbricals attach the FDP tendon to the EDC. The EDC tendon connects to the lumbricals, the dorsal interossei and to all three phalanges and is known as the extensor expansion. This arrangement allows complex movements such as the unscrewing of a pen top whilst holding the pen in one hand, but none of the movements are entirely independent because single muscles act over several joints at once. Bibliography Jacobs S. Anatomy: a dissection manual and atlas. 1996 New York: Churchill Livingston. Netter FH. Atlas of human anatomy. 1997 East Hanover, New Jersey: Novartis.
Snell RS. Clinical anatomy for medical students. 1986 Boston: Little, Brown.
Related Documents
Upper Limb
June 2020 9
Clinical Anatomy Upper Limb
June 2020 8
Joint Of Upper Limb
July 2020 10
Vishram Upper Limb And Thorax.pdf
November 2019 4
Learning Task Upper Limb And Lower Limb Muscles.docx
December 2019 18


